



It is an ‘orthodontic retainer’ that is removable and allows babies to breathe through the nose and feed by mouth. No surgery is needed for this treatment.
The oldest an OAP patient can be is 12 weeks old.
That said, the ideal starting time for treatment is between 2 and 6 weeks old.
Due to the fact that the OAP treatment is all about changing the baby’s lifestyle from what they are used to from birth to what they need to for normal craneofacial function and growth, babies 7 to 12 weeks old may still be considered, but the older the baby gets, the more resistance to initiating treatment is expected.
Yes! Stanford has created an OAP Program headed up by Dr. Choo. You can check out their website and full details at this link: https://www.stanfordchildrens.org/en/services/orthodontic-airway-plate.html
There are multiple nonprofit organizations that are specifically created to help patients who need medical care outside of their local area. Here are a few to look into:
Follow-up frequency varies depending on the baby’s clinical complexity. After an inpatient hospital stay of usually 2-3 weeks, parents are taught how to handle the OAP at home. When the parents feel competent in handling the OAP, then the patient is discharged home with the device. After the discharge, the family will be scheduled to return to the orthodontic and aerodigestive clinic at Stanford for outpatient visits every 3-6 weeks.
The time that the child will need the OAP depends on their clinical complexity. The average length of time with the OAP (from device delivery to graduation) is 3.5 months with the range of 3 weeks to 6 months.
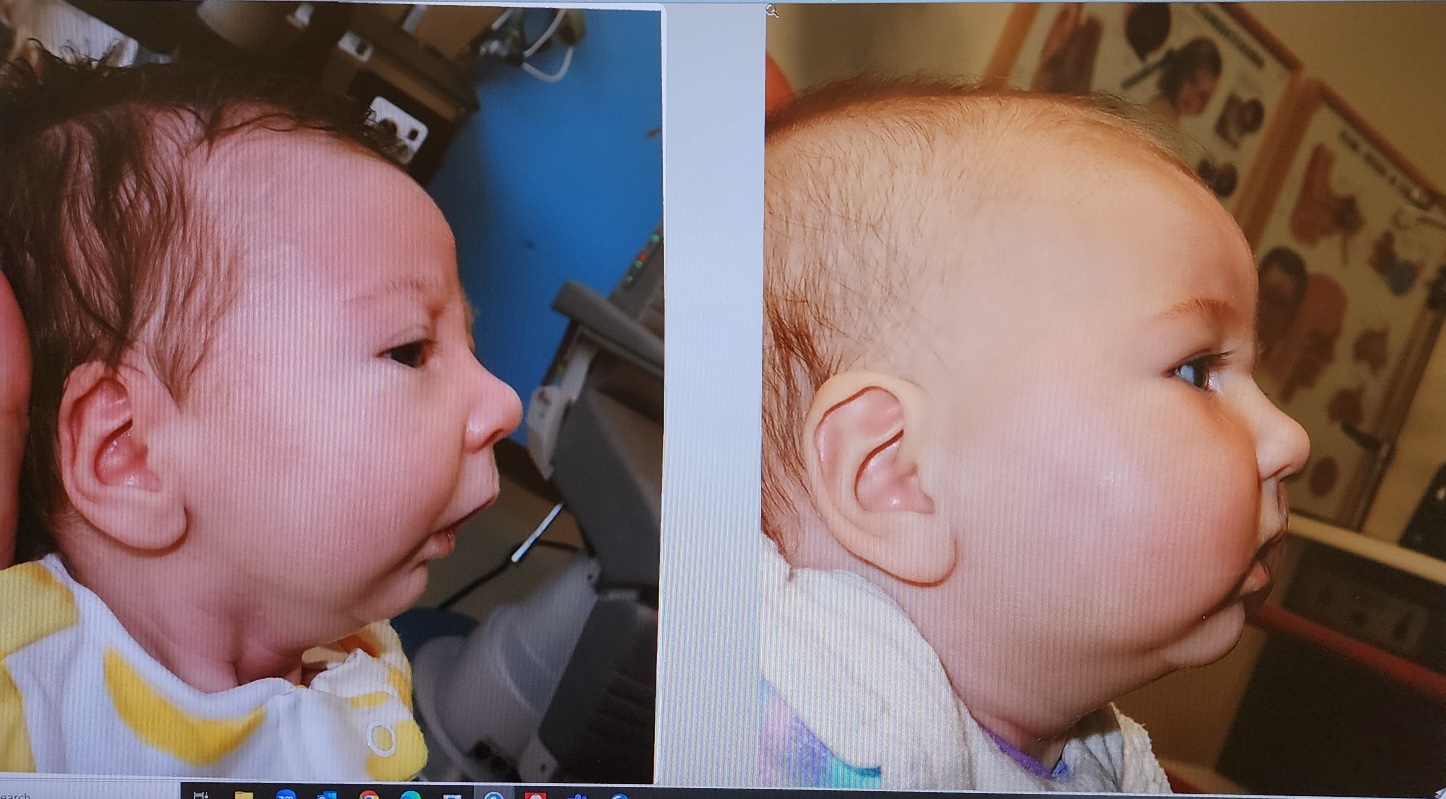
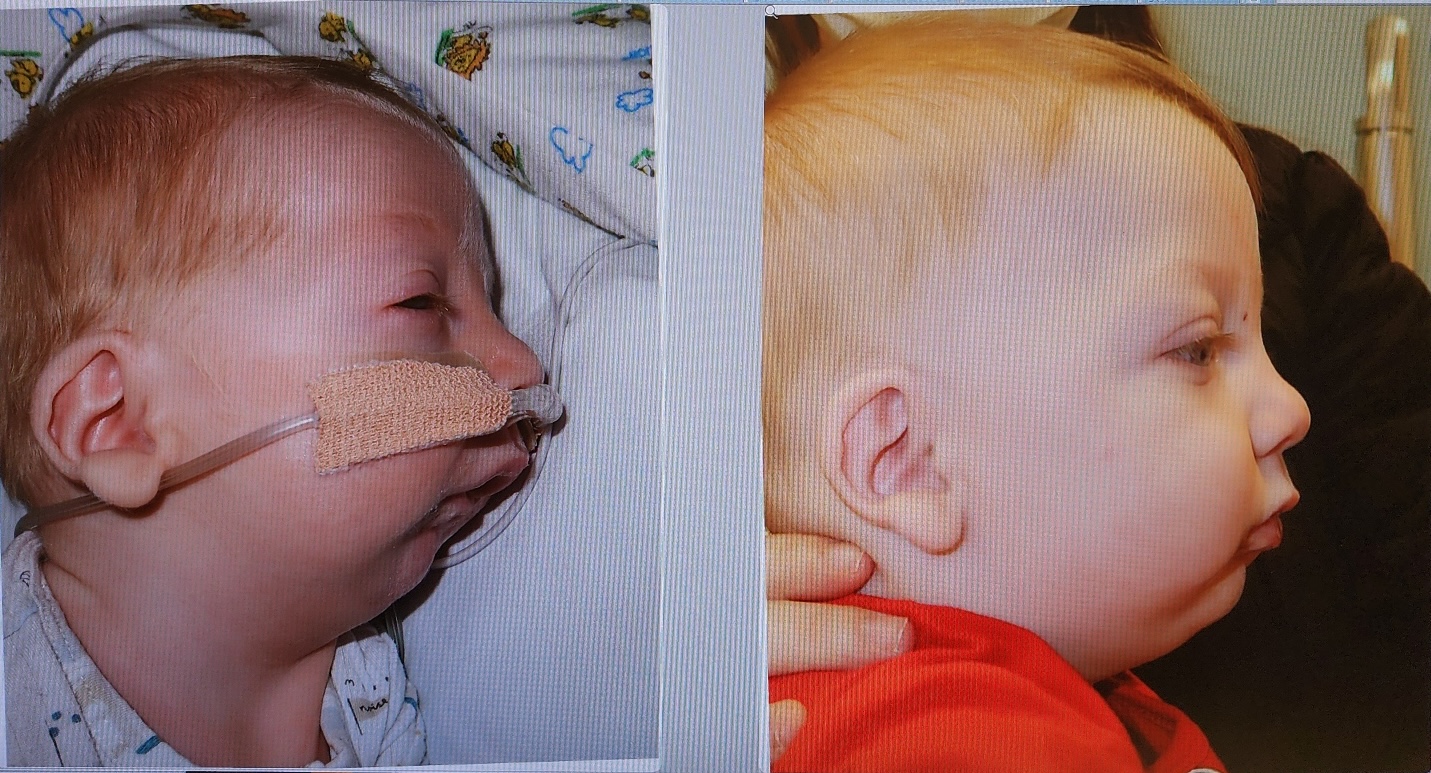
As of April 2024, 29 babies were treated with the OAP and all avoided jaw surgery. One additional baby, who was later determined to have a undiscovered neurological condition did not tolerate the attempted treatment with the OAP.
When the OAP is tolerated well by the baby during the hospital stay, none of the babies needed any airway surgery afterwards. If the baby also has a cleft palate, the cleft repair will occur in the following months (typically done at your local children’s hospital).
Sleep tests are done at several points before, during and after treatment. The first test is done prior to the OAP being delivered. The second one is done a few days after the delivery of the OAP (while inpatient), the third is done midcourse of the treatment (exact time varies), and one is done about a month after OAP graduation.
If your child has a cleft palate, repair surgery is typically done when the baby is approximately 12 months old. The baby will have graduated from OAP several months prior to the cleft palate surgery. The OAP often reduces the size of the cleft palate prior to the cleft palate surgery, making the surgery easier to complete.